|
|
Cleidocranial Dysostosis
Cleidocranial Dysplasia
General Considerations
- Rare, congenital hereditary dysostosis resulting in delayed or failed ossification of midline structures
- Especially membranous bones, but enchondral bones are also affected
- Therefore, skull and clavicles are mostly affected
- Autosomal dominant with strong familial tendencies
- Males and females have same chance of being affected
- Gene for this disorder has been found on Chromosome 6
- May also occur as a sporadic mutation
- Major changes are in the skull, clavicles and pelvis
Clinical Findings
- Large head
- Disproportionate small facial bones
- Narrow chest
- Sagging shoulders
- May be dwarfism or defective or delayed dentition
- No mental retardation
Imaging Findings
- Skull
- Intersutural bones, especially seen in the lambdoid and posterior sagittal sutures
- Large head
- Thinness and underossification of calvarium in early infancy
- Widened fontanelles and sutures with delayed closure
- Persistent metopic suture
- Midline suture in frontal bone
- Brachycephaly and prominent bossing
- Large mandible
- Nonunion of mandibular symphysis
- High narrow palate; may be cleft
- Hypoplastic paranasal sinuses, including mastoids
- Delayed or defective dentition
- Abnormally retained primary teeth
- In adulthood, petrous bones may be sclerotic
- Hypoplasia or absence of clavicles
- Clavicle normally forms from three ossification centers: sternal, middle and distal
- One or more segments in any combination may be absent
- Usually of lateral portion
- R > L
- Clavicles completely absent in 10%
- Thorax may be narrowed and/or bell-shaped
- Supernumerary ribs
- Incompletely ossified sternum
- Hemivertebrae, spondylosis (frequent)
- Exaggerated kyphosis or lordosis
- “Bone-within-a-bone”
- Delayed ossification of bones forming symphysis pubis
- Produces widened symphysis
- Hypoplastic iliac bones
- Poorly formed sacrum
- Accessory epiphyses in hands and feet are common
- Coxa vara from deformed or absent femoral necks is common
- Broad femoral head and short femoral neck
- Radius short or, rarely, absent
- Elongated second metacarpals
- Pseudoepiphyses of metacarpal bases
- Short hypoplastic distal phalanges of hand
- Pointed terminal tufts
- Coned epiphyses
Differential Diagnosis
- Widening of symphysis can be seen with bladder exstrophy
- Calvarial and clavicular changes in pyknodysostosis can be identical to cleidocranial dysostosis but bones are sclerotic in pyknodysostosis
- Short or absent radius may be seen with Holt-Oram Syndrome or TAR syndrome
- Absence or erosion of the distal clavicle can be seen with rheumatoid arthritis, hyperparathyroidism, scleroderma
- Bone-with-a-bone can be seen with osteopetrosis, Paget disease and with Thorotrast administration
- Wormian bones can bee seen with hypothyroidism, Down Syndrome, cretinism, pyknodysostosis, and osteogenesis imperfecta, but are most often a normal variant
Treatment
- Dental problems may require frequent oral care
- Genetic counseling if there is a family or personal history of cleidocranial dysostosis and the individual is planning to have children
Prognosis
- Life expectancy should be normal
- Mentation should be normal
 
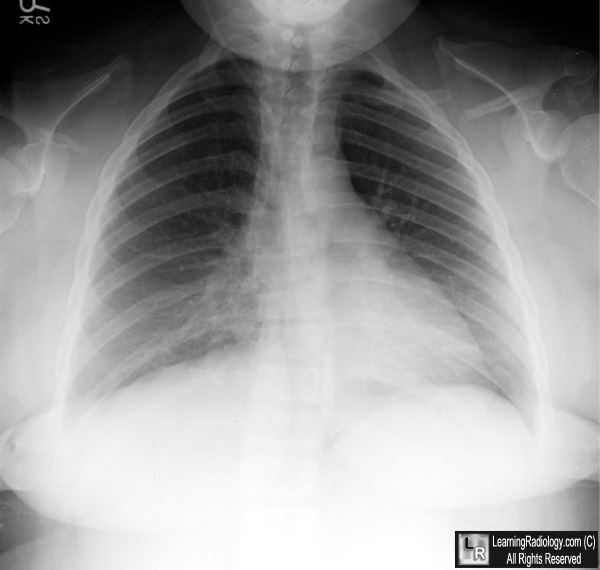
Cleidocranial dysostosis. Frontal chest radiograph on the left demonstrates complete absence of the right clavicle (white arrow) and absence of portions of the left clavicle (black arrows). The abdominal radiograph on the right shows widening of the symphysis (white arrow) and sacroiliac joints (black arrows). The iliac bones are deformed (red arrow) and there is a coxa vara deformity of both femurs.
For additional information about this disease, click on this icon if seen above.
For these same photos without annotations, click here or here
Greenfield, George 1969 JB Lippincott Radiology of Bone Diseases
Swischuk, Leonard Imaging of the Newborn, Infant and Young Child 1989 Williams&Wilkins
|
|
|

){kind=link}
{kind=link}
{kind=link}